There's a quiet crisis unfolding in exam rooms across the country, and it has nothing to do with patients.
It's the physician with fingers hovering over a keyboard. Mentally split. Half listening to the person across from them. Half composing a note that still needs to be written.
It's the 11 p.m. login to finish charting after a 10-hour shift. It's the slow realization that medicine now feels more like data entry than healing.
The paperwork problem in healthcare isn't new. But its weight has become unbearable. For every hour a physician spends with patients, they spend nearly two hours on documentation. That ratio is unsustainable. Providers know it. Their patients feel it.
The solution is the remote medical scribe.
Not an app. Not a voice-to-text shortcut. A real, trained person who works alongside the physician during every visit. They handle the documentation. The provider handles the patient. It's that clean.
What Is a Remote Medical Scribe
A remote medical scribe is a trained clinical documentation specialist. They listen to patient encounters in real time through a secure audio or video connection and record everything directly into the provider's EHR system from a remote location.
They are not transcriptionists working from a recording. They are live and active during the visit itself. The clinical narrative gets captured as it unfolds — not reconstructed hours later from memory or audio files.
The traditional model required the scribe to be physically in the room. Scrubbed in. Badge on. Standing at a workstation in the corner. The remote model removes that requirement entirely.
Through a HIPAA-compliant platform, the scribe joins the moment the provider is ready. They listen. They chart. They capture. When the visit ends, a complete clinical note is waiting for review.
Structured. Accurate. Ready to sign. The physician doesn't type a word. The patient never knows the scribe was there.
This model fits naturally into the broader category of remote healthcare solutions that modern practices are building. Telehealth expanded what's possible from a distance. Remote scribing applies that same logic to clinical documentation – the part of practice that consumes the most time and delivers the least satisfaction.
What Does a Remote Medical Scribe Do
A remote medical scribe listens to patient encounters in real time and documents everything directly into the physician's EHR from a remote location. They record the chief complaint, medical history, physical exam findings, diagnosis, treatment plan, and physician orders as the visit happens. The physician never types. The chart is complete before the next patient walks in.
Real-Time Clinical Documentation
This is the core of the job. The remote scribe listens through a secure connection. They enter information directly into the EHR as the visit happens. Not from a recording. Not after the fact. Live.
They document the chief complaint. The history of present illness. The review of systems. Physical exam findings. The physician's assessment. The plan of care. They follow the physician's natural conversational rhythm. No formal dictation required. No structured commands.
This is where remote scribing differs from standard medical transcription services. Traditional medical transcription starts with a recording submitted after the visit. It produces a text document that still needs to be manually entered into the system. A remote medical scribe works live, inside the actual EHR, building the note in real time. The result is a finished, structured, codeable document — not a raw transcript waiting to be processed.
Further Reading: What Do Medical Scribes Do in Healthcare
Pre-Charting and Visit Preparation
Many remote scribes start working before the first patient arrives. 'Pre-charting' means pulling up prior visit notes. Reviewing pending labs. Checking imaging results. Flagging outstanding referrals. Organizing the chart so the physician walks in fully prepared.
This preparation saves several minutes per encounter. Across a 25-patient day, that adds up fast. For high-volume practices, pre-charting is the difference between a schedule that flows and one that falls behind from the very first appointment.
History of Present Illness and Chief Complaint
The HPI is one of the hardest sections of any clinical note to write well. It requires more than recording the complaint. Onset. Duration. Severity. Location. Aggravating factors. Relieving factors. Associated symptoms. Relevant history. All of it must be captured and structured correctly.
A skilled remote scribe listens for these elements within a natural patient conversation. They organize them into a compliant HPI without the physician pausing to dictate. The conversation flows. The documentation keeps pace.
Physical Exam Documentation
As the physician examines the patient and narrates findings, the scribe records each system in the correct EHR fields. Cardiovascular. Respiratory. Musculoskeletal. Neurological. Dermatological. Each section gets populated with accurate clinical terminology as the exam progresses.
Nothing gets left to memory. The physician never needs to return to the keyboard before moving to the next room. The note is built section by section, in real time, as the exam happens.
Assessment, Plan, and Orders
After the exam, clinical reasoning becomes the note's most important section. The remote scribe captures the diagnosis, the differential, the treatment plan, prescribed medications, referrals, follow-up instructions, and any patient education discussed.
In some states and under appropriate supervision, scribes also enter orders for labs, imaging, and specialist referrals. This reduces the provider's administrative workload even further after the visit ends.
After-Visit Summaries and Inbox Support
Some scribing services extend beyond the visit itself. After-visit summary preparation. Prior authorization documentation. Inbox triage. Flagging patient messages, prescription refill requests, and results that need the physician's attention.
This kind of extended support overlaps with what a virtual medical assistant provides. Many practices choose services that blend both roles. The scribe handles documentation during the encounter. The virtual assistant layer handles the administrative work surrounding it.
How Does a Remote Medical Scribe Work
The workflow is simple. Most physicians are comfortable with it within the first few days.
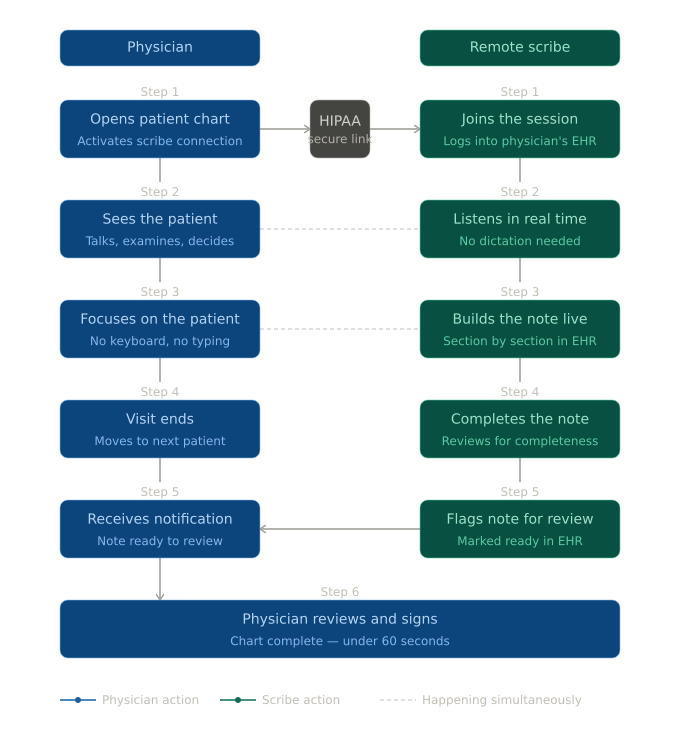
The physician opens the patient chart and activates the scribe connection. This happens through a dedicated tablet, a smartphone, or a clip-on microphone linked to the scribe platform. The remote scribe, already logged into the physician's EHR, joins through a HIPAA-compliant audio link. Some setups include video. Others use audio alone.
The physician sees the patient as they normally would. They talk. They examine. They listen. They make clinical decisions. The scribe works quietly in the background. Section by section, the note gets built in real time. No formal dictation. No commands. No pausing mid-visit to say "new paragraph".
When the visit ends, the scribe completes the note and performs a quick review for completeness. They flag it in the EHR for the physician's signature. The physician reviews it — often in under a minute — and signs. The chart is done. The room is clear. The physician walks to the next patient without carrying the weight of an unfinished note.
Most remote scribes work inside the major EHR platforms: Epic, Cerner, Athenahealth, eClinicalWorks, DrChrono, Kareo, and others. No new software. No system changes. No IT project. The scribe adapts to the practice's existing tools.
10 Benefits of a Remote Medical Scribe
The case for remote scribing is not theoretical. It is documented across thousands of practices. Here are the 10 benefits that show up most consistently:
1. Dramatically Less Time Spent on Documentation
Physicians spend 15 to 17 minutes documenting a single patient encounter. Across 20 to 30 patients a day, that is hours. Every day. Added to the end of an already long shift, or carved out between rooms, slowing everything down.
A remote scribe removes that time entirely. Notes get built during the visit. By the time the last patient leaves, the chart is done. Physicians report cutting documentation time by 50 to 70 percent. Many describe finishing their day on time for the first time in years.
2. More Patients Seen Per Day
Documentation is a bottleneck. Remove it, and the schedule opens up.
Physicians no longer need to build extra time into appointment slots for charting. They move between rooms without stopping. They stay on schedule. Practices report 15 to 25 percent increases in daily patient volume after adding remote scribes. Not because providers are rushing because they are no longer losing time between visits to a keyboard.
3. Consistently Higher Note Quality
At the end of a long day, a tired physician writes tired notes. Attention narrows. Shortcuts appear. Complex visits get compressed into documentation that is technically sufficient but clinically incomplete.
A dedicated remote medical scribe does not have this problem. Their focus is documentation. Their sole job is to capture the visit accurately. From the first encounter of the day to the last, they produce thorough, structured notes. Quality does not decline as the schedule wears on. That consistency matters — for patient care, for coding, and for compliance.
4. Real Reduction in Physician Burnout
More than 60 percent of physicians report symptoms of burnout. EHR documentation is the leading cause. That is not speculation — it appears in study after study across nearly every speciality.
Remote scribing removes the most persistent daily source of that frustration. Physicians who work with remote scribes describe feeling like physicians again. More present during visits. Less depleted after them. More connected to the work that brought them into medicine.
5. Better Visits for Patients
Consider two versions of a medical appointment. In the first, the doctor types through the entire visit. Eye contact is rare. The conversation feels rushed and transactional.
In the second, the doctor looks up. Listens. Responds. The visit feels like a real conversation between two people. Remote scribing makes the second version the standard. When the chart is handled, the physician gives the patient their full attention. Patients notice. Satisfaction scores reflect it. Trust builds faster. Treatment adherence improves.
6. Lower Overhead Than In-Person Scribing
Hiring an on-site scribe costs more than the hourly wage. There is the physical space in the exam room. The equipment. The scheduling complexity. The coverage gaps when the scribe is unavailable. Remote scribing eliminates most of that overhead.
The scribe works from their own location on their own setup. Services scale up or down without the friction of in-person staffing. For independent practices and smaller groups, this cost structure makes professional scribing financially realistic in a way in-person scribing never was.
7. Trained for Your Specialty
Remote scribing is not one-size-fits-all. Scribes train in speciality-specific terminology, documentation standards, and coding requirements. A psychiatrist managing medication adjustments needs very different documentation than an orthopaedic surgeon recording post-operative care.
A skilled remote medical scribe adapts to the clinical language and workflow of the speciality they support. The physician does not change how they work. The scribe learns to match it.
8. Faster Billing and Fewer Denied Claims
Documentation quality has a direct impact on revenue. Vague or incomplete notes lead to downcoding, claim denials, and audit exposure. When a remote scribe produces thorough, well-structured notes, the documentation supports accurate coding from the start.
Paired with strong medical billing solutions, this improvement in note quality leads to better collection rates, fewer claim corrections, and less back-and-forth with payers. The revenue cycle moves faster because the documentation feeding it is cleaner.
9. Works Inside the Systems You Already Use
Practices worry about disruption when considering any new service. With remote scribing, that concern rarely materializes.
Remote scribes work inside the practice's existing EHR. No new software to implement. No staff retraining. No IT project to manage. The scribe learns the system the practice already uses — whether that is Epic, AthenaHealth, eClinicalWorks, or another platform — and builds documentation within it from day one.
10. A Platform for Practice Growth
Remote scribing is an entry point into something larger. Once a practice experiences clean, same-day documentation, the appetite for broader operational support grows naturally.
That might mean adding a virtual medical assistant to manage scheduling, referrals, and patient communications. It might mean integrating stronger medical billing solutions to connect documentation quality directly to revenue performance. It might mean expanding telehealth, knowing the documentation infrastructure is already in place to support it.
Remote scribing does not just solve the note problem. It builds the operational foundation a growing practice needs to run at a higher level.
Is a Remote Medical Scribe Right for Your Practice
Most practices dealing with documentation fatigue are a strong fit. Some situations make it especially clear.
Physicians finishing charts after hours have the most immediate need. Notes are not getting done during the day because there is no time. The cost falls directly on the physician — lost evenings, reduced recovery, accumulated exhaustion. Remote scribing addresses this at the source.
High-volume practices in urgent care, primary care, or speciality settings see large, fast returns. Seeing 25 to 30 patients a day means a 5-minute reduction per encounter gives back more than two hours to the physician's day.
Practices where screen-heavy visits are hurting patient satisfaction will see fast, visible improvement. Practices where documentation gaps are creating billing or compliance problems benefit both operationally and financially.
Solo practitioners and two-provider groups often assume remote scribing is built only for larger organizations. It is not. Many find it pays for itself quickly — particularly when better documentation leads to cleaner coding and faster reimbursement.